Authors: Scott L. Bruce, EdD, AT, ATC
Siobhan Fagan M.Ed, AT, ATC, CSCS
Cody Cummins, AT, ATC
Brooke Kidd, AT, ATC,
Jasmin Harvey, ATC
Wright State University
Corresponding Author:
Scott L. Bruce, EdD, AT, ATC
Assistant Professor/Director of Research
Wright State University
3680 Colonel Glenn Hwy
Dayton, OH 45435
937-245-7622
scott.bruce@wright.edu
Scott Bruce is an Assistant Professor and the Director of Research for the Athletic Training Program at Wright State University.
Effect of Therapeutic Tape on Upper Extremity Reaction Time
ABSTRACT
The athletic training literature is lacking when comparing therapeutic tapes applied to the shoulder. The effect of these tapes on pain and range of motion have been studied, but their effect on reaction time has not. The purpose of this study was to determine whether the use of therapeutic taping has an effect on shoulder reaction time as assessed on a Dynavision™ unit. A single-blind, randomized control trial design was implemented. Participants included 23 male and 33 female, physically-active, college-aged, volunteer students. Baseline tests were performed on the Dynavision™ consisting of one warm-up activity and three reaction time tests. Participants returned a minimum of two weeks later and were randomly assigned to receive either Kinesio Tape®, RockTape or a sham tape applied to the slowest, baseline tested, shoulder. All tapes were applied by the same certified athletic trainer trained in both Kinesio Tape® and RockTape applications. Participants were blind folded to prevent them from seeing which tape was being applied. At the conclusion of the tape application participants rested for a minimum of 30 minutes, as per manufacturers’ recommendations, before repeating the same set of Dynavision™ tests. A chi-square test found no statistical differences across the three tape groups (2 = 0.426, p = 0.808). A paired t-test was used to assess each of the five different testing conditions for both shoulders of which 18 were the three different taped conditions. Although the RockTape condition was found to have the greatest difference in mean time across all three tests, only 4 of the 18 taped conditions assessed reached statistical significance. These results suggest, regarding shoulder reaction time, RockTape may be more beneficial than Kinesio Tape® or a sham tape.
Keywords: Therapeutic taping, Dynavision, Kinesio Tape®, Rock Tape, sham tape, reaction time
INTRODUCTION
The available literature related to therapeutic tape, such as Kinesio Tape® and RockTape, and its use with upper extremity dysfunction is limited. Investigators have examined the use of therapeutic tapes verses controls, or sham taping, for musculoskeletal injuries, inflammation, pain relief, and support (Aarseth, Suprak, Chalmers, Lyon, & Dahlquist, 2015; Alam, Malhotra, Munjal, & Chachra, 2015; Drouin, McAlpine, Primak, & Kissel, 2013; Fu, Wong, Pei, Wu, Chou, and Lin, 2008; Mostafavifar, Wertz, & Borchers, 2012; Ronning, 2015; Thelen, Dauber, & Stoneman, 2008; Williams, Whatman, Hume, & Sheerin, 2012). Kinesio Tape® presents several claims on their web site regarding facilitating healing, providing support to the body’s tissues, and manipulating soft tissue (Kinesio Taping Association International, 2016) RockTape claims their product is able to aid in edema control and improve proprioception (RockTape USA, 2016).
Several studies have examined Kinesio Tex Tape® applied to the shoulder and its effect on several independent variables such as: pain, proprioception, range of motion, strength, grip strength, peak torque, athletic performance, and disability scores (Aarseth, Suprak, Chalmers, Lyon, and Dahlquist, 2015; Alam, Malhotra, Munjal, and Chachra, 2015; Drouin, McAlpine, Primak, and Kissel, 2013; Mostafavifar, Wertz, and Borchers, 2012; Thelen, Dauber, and Stoneman, 2008; Wells Hoffman, and Beyer, 2014). Each of these studies found little to no evidence to support any positive effects of Kinesio Tape® use on shoulder performance. Only one scientific study was found utilizing RockTape applied to the shoulder. Pain and range of motion were the parameters studied and it was determined that RockTape had no positive or negative effects (Ronning, 2015).
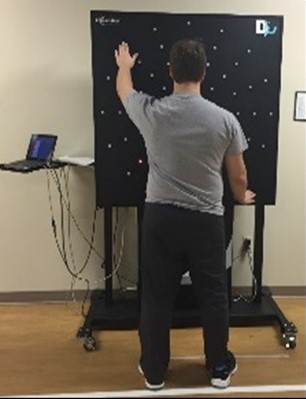
The Dynavision™ D2 Visuomotor Training Device has been used to assess reaction time, depth perception, visual acuity and hand-eye coordination (Clark, Ellis, Bench, Khoury, & Graman, 2012; Clark Graman, and Ellis, 2015; Wellset al., 2014). The Dynavision™ is a large, (4’ X 4’), board with a series of 64 lights arranged in a series of 5 concentric circles. The unit is a visual motor and neuro-cognitive rehabilitation training device used by rehabilitation and performance enhancement specialists in medical, athletic, and tactical settings (Dynavision, 2016). The unit permits the clinician to either assess or train the patient for reaction time, as well as central and peripheral vision. Use of the Dynavision™ can be individualized with the lights illuminating either red or green, and the subject is instructed to react quickly by hitting the lights as they light up or avoiding specific lights. A small screen in the middle of the board known as the tachistoscope (T-scope) can show numbers, letters, words, or scrolling text to further challenge the participant cognitively while acting/reacting to the illuminating lights (Clark, Ellis, Bench, Khoury, and Graman, 2012; Clark et al., 2015; Dynavision, 2016).
The Dynavision™ has been found to be reliable with ICC values ranging from 0.63 to 0.92 (Clark et al., 2012; Clark et al., 2015; Wells et al., 2014). A literature review found no peer-reviewed studies published examining the use of therapeutic tape applied to the shoulder and the effect these tapes may have on reaction time. The purpose of this study was to determine whether therapeutic tape has an effect on reaction time as assessed using a Dynavision™ D2 unit.
METHODS
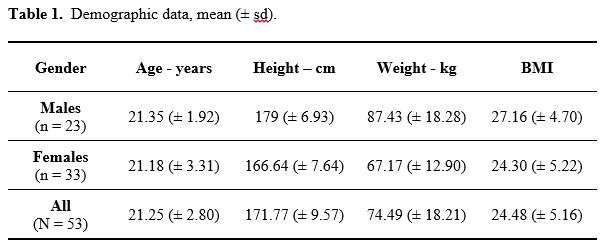
The sample for this study were 56 healthy, physically active, college aged volunteers (23 males, 33 females). Demographic data for this group is provided in Table 1. Participants were excluded if they had a shoulder injury within the past six months or if they were a student-athlete of a predominately overhead sport, (baseball/softball, tennis, swimming/diving etc.).
Dynavision™ Testing
Baseline tests were conducted on the Dynavision™ without tape, so participants functioned as their own controls. Participants stood 14 inches from the Dynavision™ unit and it was adjusted for each individual’s height. From their reflection on the unit’s T-scope screen the participant notified the athletic trainer when the bridge of their nose was at the top of the screen (Clark et al., 2012; Clark et al., 2015).
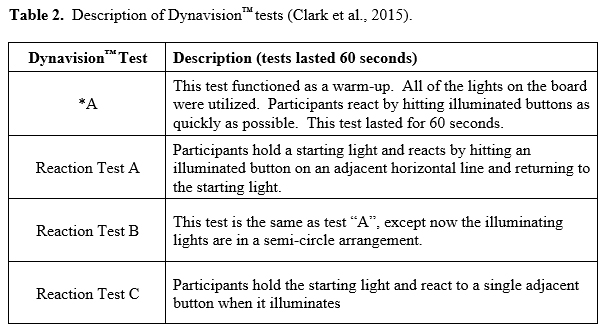
A script of instructions for each of the four Dynavision™ tests was read to the participants by an athletic trainer prior to the performance of each test. The first test was a warm-up activity (*A test). The other three tests were all reaction time tests (Figure 1). The four tests are summarized in Table 2. Each of the three reaction time tests lasted for at least seven repetitions with the 5 fastest repetitions used for the analysis (Clark et al., 2012; Clark et al., 2015).
Therapeutic taping
Participant’s returned a minimum of two weeks after taking the Dynavision™ baseline test (mean 18.85 days, ± 7.11) to be re-tested under one of the three tape conditions (Kinesio Tape®, RockTape, or a sham tape group) to which they were randomly assigned. The taped arm was the arm with the slowest average reaction time, determined from baseline data analysis. Participants were blindfolded to prevent them from knowing the type of tape applied to their shoulder. The same certified athletic trainer, trained in both Kinesio Tape® Level 1 & 2, and RockTape Basic & Performance Functional Movement Techniques, applied all of the tapes to the participants. After the tape was applied, the participant’s shirt sleeve was pulled down over the tape to hide the type and brand of tape that had been applied.
Therapeutic and sham tapes were applied in the same manner and the same color of tape was utilized for all applications (Mueller MTAPE ®Athletic Tape was used as the sham tape). After each subject was blindfolded, adhesive spray was applied using Cramer Q.D.A. ® to ensure adhesion. A strip of tape approximately 30 cm was cut. The base of the tape was applied over the acromioclavicular joint. The anterior and posterior heads of the deltoid were identified and the tails of tape were applied over each head while the subject was placed in the direction of maximal range of motion per head (Figure 2). Once applied, the tape was rubbed for 15 seconds to increase adhesion. Following tape application, as per the manufacturers’ recommendation, participants rested for a minimum of 30 minutes (mean = 53.64 mins. ± 24.83) before performing the same Dynavision™ tests that were done at baseline (Dynavision, 2016; RockTape USA, 2016).

RESULTS
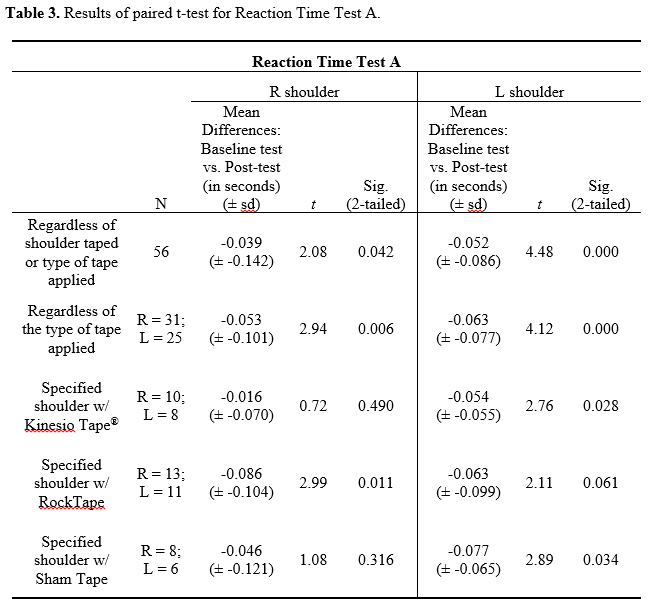
For all statistical assessments, the alpha level was set a priori at less than or equal to 0.05. A chi-square (c2) test found no statistical differences across the three tape groups baseline times (c2 = 0.426, p = 0.808). The mean differences in reaction time from baseline to the post-test were calculated. A negative number indicated a reduction in post-test time compared to the baseline test. Results from Reaction Time Test A found statistically significant results for the conditions regardless of shoulder taped or the type of tape applied (Table 3). Examining the three different tape conditions found the RockTape condition for the right shoulder to not only have the greatest difference in mean time, but also it was found to be statistically significant. For the left shoulder, the sham taping condition had both the greatest mean time difference and was statistically significant. The Kinesio Tape® condition for the left shoulder had the slowest mean time difference, but was found to be statistically significant.
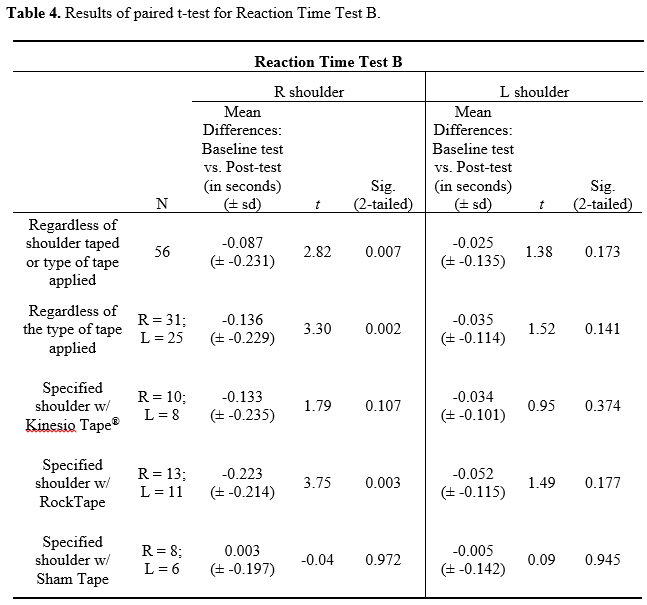
For the Reaction Time Test B condition, only the right shoulder was found to be statistically significant for the conditions regardless of shoulder taped or the type of tape applied (Table 4). For the three taped conditions, RockTape again was found to have the greatest mean time difference and statistical significance for the right shoulder. The RockTape condition for the left shoulder had the greatest mean time difference, but it was not statistically significant.
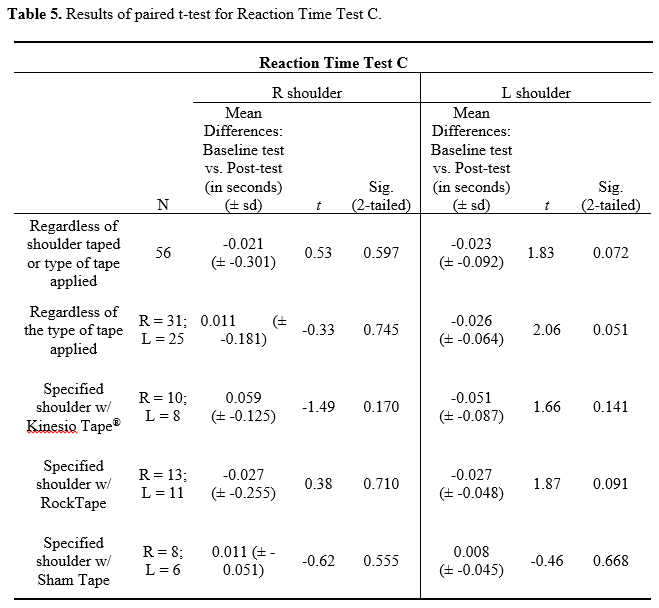
For Reaction Time Test C, the RockTape condition had the greatest mean time difference for both the right and the left shoulder; however, neither of these results were statistically significant (Table 5).
DISCUSSION
The purpose of this study was to determine whether therapeutic tape had an effect on reaction time as assessed using a Dynavision™ D2 unit. There were five different testing conditions that were assessed: for both shoulders and for all three forms of taping, of which 18 were the three different taped conditions. The RockTape condition had the greatest mean time difference for upper extremity reaction time when assessed using a Dynavision™ unit. Statistical significance was only found in four of these 18 cases. The presence or absence of statistical significance does not always equate to clinical significance and this may be the case with this study. Caution should be used when applying these results to student-athletes. None of the participants were active intercollegiate student-athletes at the time of this study, and only two were former intercollegiate student-athletes. A majority of the participants were former interscholastic student-athletes. Repeating this study with either current intercollegiate or interscholastic student-athletes as participants may provide valuable data and insight.
This study was not without its limitations. Although a priori statistical power of 90% provided a recommended sample of 45 participants, the sample of 56 obviously strengthened the study from the outset however, stratification of the data and cases obviously weakened the study. Repeating the study with consideration for the stratification and determining the a priori power for the conditions assessed would aid in improving the study.
To reduce the potential for a practice effect by the participants on the Dynavision™ it was established that a minimum of two weeks of waiting occurred between the baseline and the post-test. With a mean of 18.85 days between baseline testing and post-testing the potential for a practice effect was minimized. Although it cannot be guaranteed that the participants may have engaged in other activities that may have directly or indirectly improved their reaction times.
CONCLUSIONS AND APPLICATIONS IN SPORT
There is an absence of high quality research related to the various types of therapeutic tapes. This study was able to demonstrate a clinical improvement in Dynavision™ reaction time for those participants wearing RockTape compared to those wearing Kinesio Tape® or a sham taping. While only a few of the results were determined to be statistically significant, the fact that Dynavision™ reaction time improved should not be discounted.
Declaration of Conflicting Interests
The Authors declares there are no conflicts of interest.
REFERENCES
1. Aarseth, L. M., Suprak, D. N., Chalmers, G. R., Lyon, L., & Dahlquist, D. T. (2015). Kinesio tape and shoulder-joint position sense. Journal of Athletic Training, 50(8), 785-791.
2. Alam, S., Malhotra, D., Munjal, J., & Chachra, A. (2015). Immediate effect of Kinesio taping on shoulder muscle strength and range of motion in healthy individuals: A randomised trial. Hong Kong Physiotherapy Journal, 33(2), 80-88.
3. Clark, J. F., Ellis, J. K., Bench, J., Khoury, J., & Graman, P. (2012). High-performance vision training improves batting statistics for University of Cincinnati baseball players. PloS one, 7(1), e29109.
4. Clark, J. F., Graman, P., Ellis, J. K., Mangine, R. E., Rauch, J. T., Bixenmann, B., . . . Myer, G. D. (2015). An exploratory study of the potential effects of vision training on concussion incidence in football. Optometry and Visual Performance, 3(1).
5. Drouin, J. L., McAlpine, C. T., Primak, K. A., & Kissel, J. (2013). The effects of kinesiotape on athletic-based performance outcomes in healthy, active individuals: a literature synthesis. Journal of the Canadian Chiropractic Association, 57(4), 356-365.
6. Dynavision. (2016). Experience the proven power of Dynavision! . Retrieved from http://www.dynavisioninternational.com/
7. Fu, T.-C., Wong, A. M., Pei, Y.-C., Wu, K. P., Chou, S.-W., & Lin, Y.-C. (2008). Effect of Kinesio taping on muscle strength in athletes—a pilot study. Journal of Science and Medicine in Sport, 11(2), 198-201.
8. Kinesio Taping Association International. (2016). What is the Kinesio taping method? Retrieved from https://kinesiotaping.com/about/what-is-the-kinesio-taping-method/
9. Mostafavifar, M., Wertz, J., & Borchers, J. (2012). A systematic review of the effectiveness of Kinesio taping for musculoskeletal injury. Physician & Sportsmedicine, 40(4), 33-40. doi:10.3810/psm.2012.11.1986
10. RockTape USA. (2016). RockTape: Go stronger, go longer. Retrieved from http://www.rocktape.com/
11. Ronning, R. (2015). The Effects of Kinesiology Tape on Pain and Range of Motion for Individuals with Shoulder Pain. (Master of Science – Human Performance), University of Wisconsin-La Crosse, La Crosse, WI.
12. Thelen, M. D., Dauber, J. A., & Stoneman, P. D. (2008). The clinical efficacy of kinesio tape for shoulder pain: a randomized, double-blinded, clinical trial. journal of orthopaedic & sports physical therapy, 38(7), 389-395.
13. Wells, A. J., Hoffman, J. R., Beyer, K. S., Jajtner, A. R., Gonzalez, A. M., Townsend, J. R., . . . Fragala, M. S. (2014). Reliability of the Dynavision™ D2 for assessing reaction time performance. Journal of Sports Science and Medicine, 13, 145-150.
14. Williams, I., Whatman, C., Hume, P. A., & Sheerin, K. (2012). Kinesio taping in treatment and prevention of sports injuries. Sports Medicine, 42(2), 153-164. doi:10.2165/11594960-000000000-00000
