Submitted by Guy Wadas, MS, Southern Utah University and Mark DeBeliso, PhD, Southern Utah University
ABSTRACT
PURPOSE: This study investigated the prevalence of disordered eating behaviors among male high school cross country runners. The study identified behaviors and feelings about being an athlete, and determined relationships between motivations to exercise and disordered eating behaviors. METHODS: Sixty-eight male high school cross country runners from 12 high schools in one urban school district completed three questionnaire packets on one occasion pre-season. The EAT-26 questionnaire was used to determine prevalence of disordered eating. The ATHLETE questionnaire was used to determine psychological factors for relationships with disordered eating. The EMI-2 was used to determine motivations to exercise and the relationship to disordered eating. EAT-26 scores and data from the EMI-2 and ATHLETE questionnaires were analyzed via a Pearson Correlation Coefficient. RESULTS: A modest positive relationship existed between exercising for disordered eating behaviors versus exercising for weight management (r = 0.31: p < 0.05), the Your Body in Sports subscale (which measured drive for thinness and performance) (r = 0.36: p < 0.05), and the Feelings about Performance subscale (or Performance Perfectionism) (r = 0.26: p < 0.05). CONCLUSIONS: Risk factors associated with eating disorders exist in high school male cross country runners. Underreporting and lack of recognition of disordered eating may affect prevalence rates. Recommendations include a longitudinal study of male high school runners across the school year to determine relationships with the timing of questionnaire administration. APPLICATIONS IN SPORT: Disordered eating behaviors should be acknowledged as more than a “female only” issue. Parents, teachers, coaches, and athletic trainers may be better able to understand and help male athletes with disordered eating behaviors or an active eating disorder.
INTRODUCTION
According to the National Association of Anorexia Nervosa and Associated Disorders (2010), “up to twenty-four million people of all ages and genders suffer from an eating disorder (anorexia, bulimia and binge eating disorder) in the U.S.” (p. 1). Adolescents and young adults are a high-risk group (1, 2). Some researchers have suggested that the percentages of eating disorders in athletes may be greater versus non-athletes (31). Further, the research suggests that athletes in sports such as distance running or sports that require thinness are more at risk for eating disorders (10, 32, 36), while others suggest that this may vary by gender (19, 22).
A number of studies have focused on the prevalence of eating disorders among athletes (13, 31, 35). Gender, race, sports that require a thin or lean body type, competition level and age, performance pressure, social pressure, and personality characteristics are related to disordered eating in athletes (7, 13, 14). The research examining the relationship between the risk factors for eating disorders and athletes in general is equivocal (13, 18, 31). Some studies have determined factors that may provide a greater risk of disordered eating among athletes, while other studies have determined that some factors are not predictive of greater risk in athletes. Regardless of which risk factors are related to eating disorders in athletes, the prevalence of eating disorders in female athletes is unequivocal (13, 21, 32) .
The prevalence of eating disorders in male athletes is unclear. Eating disorders in male athletes may be more prevalent than previously thought, with the sport environment actually increasing the risk (10, 13, 30). The existence of eating disorders among male athletes may be more prevalent in aesthetic sports such as cross country and marathon running, which are similar to the categories for female athletes (3). In general, research suggests that eating disorders are a rapidly growing phenomenon among male athletes. Male risk factors for eating disorders may be different versus females, and the natural course of eating disorders may differ between men and women (4, 8, 38). Patel et al. (28) noted that eating disorders in male athletes are relatively uncommon and the sports where eating disorders exist are where control behaviors are prominent. Female athletes are more at risk than males (22, 28, 31). In summary, there is a paucity of and conflicting research available on the prevalence of eating disorders and symptomatology in male athletes.
Purpose
The purpose of this study was to investigate the prevalence of disordered eating behaviors in male high school cross country runners, identify risk factors, and to relate the motivations to exercise with responses from the Eating Attitudes Test-26 (EAT-26), the ATHLETE questionnaire, and the Exercise Motivations Inventory-2 (EMI-2).
METHODS
Participants
The runners were selected from 12 of the thirty-two public high schools in the local school district sponsoring sports teams. The school district is located in the southwestern part of the United States and is comprised of 49 public high schools considered a large urban school system. Some of the public schools within the school district did not sponsor athletic programs. Overall, 68 high school male cross country runners completed the EAT-26, EMI-2, and the ATHLETE questionnaires. Of the 68 participants, 48 (70.6%) were White, while only 2 (2.9%) were African-American.
All participants were current members of a high school cross-country team. The participants were in grades 9-12 and between the ages of 14-18. The Mage was 15.9 with a SD of 1.0. The most common ethnicity was White (70.6%), followed by Asian-American and Pacific Islander (11.8%), 2 or more races (8.8%), Hispanic and Latino (5.9%), and African-American (2.9%). Table 1 shows the demographic information.
Instrumentation
Questionnaires were used to gather demographic and health history information, feelings and behaviors about being an athlete, prevalence and symptoms of disordered eating behaviors and eating attitudes, and motivations for exercise. The questionnaires included the EAT–26 (9), ATHLETE Questionnaire, and Exercise Motivation Inventory–2 (EMI–2).
Several self-report attitudes toward eating questionnaires assess eating disorder prevalence and symptoms in clinical and nonclinical populations. The most common measure and most often used among athletic populations is the EAT-26 (8, 13, 22, 23, 32). The EAT–26 assesses the likelihood that an athlete would be susceptible to disordered eating. The questionnaire uses a 6-point Likert scale ranging from “never” to “always”. The items marked “never”, “rarely”, or “sometimes” are scored 0, “often” is scored 1, “usually” is scored 2, and “always” scored 3. The sum of the points determines the likelihood of disordered eating. A cut-off score of 20 indicates the athlete could be at risk for disordered eating (the higher the score, the greater the risk of disordered eating). Despite the limitations and gender biases, the Eating Attitudes Test is one of the most widely used tools showing merit in diagnosing eating disorders among men (37).
A more recently developed measure is the ATHLETE questionnaire, designed to assess the psychological predictors of disordered eating in athletics. The ATHLETE questionnaire is useful in studying the etiology of disordered eating in athletes (15). The ATHLETE questionnaire is composed of 40 items in a 5-point Likert Scale divided among subscales. The subscales include Feelings about Being an Athlete (Athlete Identity), Your Body and Sports (Drive for Thinness and Performance), Feelings about Performance (Performance Perfectionism), Support from Your Coach and Teammates (Team Trust), Feelings about Your Body (Social Pressure on Body Shape), and Feelings about Eating (Social Pressure on Eating). All subscales were used in the present study. The values assigned range from “Strongly Disagree” = 1 to “Strongly Agree” = 5. Boldface items were reversed scored, from “Strongly Disagree” = 5 to “Strongly Agree” = 1. A score for each factor is determined by the sum of the values and divided by the number of items per factor. The scoring of each subscale reflects higher scores with a greater degree of the construct being assessed (15).
The Exercise Motivations Inventory–2 (EMI–2) is a 51-item questionnaire developed concerning the reasons people give for exercising or reasons people might begin exercising.
The EMI-2 was developed as a means of assessing participation motives in order to examine such issues as the influence of motives on exercise participation, how such motives might influence the choice of activities undertaken, how affective responses to exercising may be influenced by reasons for exercising and how involvement in physical activity might have a reciprocal influence on participation motives(20).
Values assigned to the Likert scales include “Not true at all for me” = 0 to “Very true for me” = 5. The score for the questionnaire is calculated by totaling the score for each subscale and dividing by the number of items in each subscale. Stress Management, Revitalization, Enjoyment, Challenge, Social Recognition, Affiliation, Competition, Health Pressures, Ill-Health Avoidance, Positive Health, Weight Management, Appearance, Strength and Endurance, and Nimbleness comprise the 14 subscales of the EMI-2 (20). The weight management and appearance subscales were used in the present study. Sample items associated with the weight management and appearance subscales include “Because exercise helps me to burn calories” and “To have a good body”, respectively(20).
Procedures
A Notification of Action Research Project was submitted to the school district in order to obtain permission to conduct the study in the schools. Southern Utah University Institutional Review Board (IRB) certification and consent was obtained in order to begin collection of data. After permission was received from the school district and the IRB, contact with the athletes was made through the administration and coaching staff of high schools in the local area. Each principal and coach was provided information on the purpose of the study and the instrumentation to be administered. A consent form and informational letter detailing the purpose of the study was sent home with each athlete in order to obtain permission from parents or guardians to use the data from the questionnaires in this study. Since the participants were minors, informed consent was obtained from parents and assent forms were collected from the participants prior to gathering data.
Full instructions were provided on the first page of the questionnaire booklet and any further questions were addressed prior to assessment. The questionnaire packets were distributed by the coach and collected by the coach. The consent forms and completed questionnaires were sealed in separate envelopes. The study required approximately 20 to 30 minutes to complete.
Statistical Analysis
The Pearson correlation coefficients were determined between the intra-individual characteristics and eating disorders as measured on the ATHLETE and EMI–2 with the overall score on the EAT-26. A p-value less than 0.05 was considered significant and the SPSS 19 (PASW Statistics 19) computer program was used for statistical analysis. The “Your Body and Sports”, “Feelings About Eating”, “Feelings About Your Body”, “Feelings About Performance”, “Support From Teammates”, and “Feelings About Being An Athlete” subscales of the ATHLETE questionnaire were used. The EMI–2 subscales used were “Appearance” and “Weight Management”.
Athletes who scored a 14 or higher were included in the disordered eating group. A score of 14 was selected because this score is one standard deviation above the mean, according to population norms (M = 6.97; SD = 6.99) (5, 6). Patterns of disordered eating behaviors and disordered eating disturbances or diagnoses can be viewed along a continuum or spectrum. Including athletes in this group expands the population of athletes in the present study to those with a clinical definition of an eating disorder and those with eating behaviors that remain subclinical, but may be detrimental to the health of the athletes (5, 18).
RESULTS
The mean EAT-26 score for all participants was 6.0 (SD = 6.5). The results show that three of the 68 (4.41%) male high school cross country runners scored 20 or higher, indicating at risk for disordered eating. An additional 13.2% (n = 9) met the cut-off score of 14 for disordered eating behaviors, one standard deviation above the mean for population norms (5, 6). Figure 1 shows the breakdown of EAT-26 scores for the male high school cross country runners (N = 68). The present study examined the intra-individual characteristic associations of the ATHLETE and EMI-2 questionnaires with the EAT-26 scores for the participants. Table 2 shows the mean score, standard deviation, and a sample item from the questionnaires for all subscales. The “Your Body and Sports” subscale scores showed that 5.9% (n = 4) runners scored 4 or higher on the items related to this subscale. The subscale, “Your Body and Sports” measures drive for thinness and the relationship to the performance in athletes. The “Physical Appearance” subscale scores of the EMI-2 questionnaire showed 12 of 68 (17.6%) of male cross country runners scored 4 or higher on the items related to this subscale, indicating that the item was a strong motivation to exercise. Thirteen of 68 (19.1%) of male cross country runners scored 4 or higher on the items related to the “Weight Management” subscale of the EMI-2, indicating that the item was a strong motivation to exercise.
Table 3 shows the number and percentages of responses regarding desired weight on the ATHLETE questionnaire. The results show that 26 of 68 male runners (38.2%) reported a desire to gain weight. The results also demonstrate that there was dissatisfaction with current weight in that nearly 65% of the male runners desired a weight change.
Table 4 shows the correlation coefficients between the EAT-26 and the subscales of the EMI-2 and the ATHLETE questionnaires. There was a positive correlation between “Your Body and Sports” subscale and the EAT-26 score, r = .36, p = .003, indicating that as the runners felt more strongly about the items, the EAT-26 score was greater. Overall, there was a moderate positive correlation between the “Your Body and Sports” subscale of the ATHLETE questionnaire and the EAT-26 score.
The Pearson correlation coefficient for the “Weight Management” subscale and the EAT-26 score was r = .31, p = .011. This suggests that as the motivation to exercise for weight management purposes increases, the more likely the association with disordered eating behaviors.
There was a modest positive correlation (r = .26, p = .030) for the “Feelings about performance” subscale of The ATHLETE Questionnaire and the EAT-26 score. This suggests a positive relationship between the items of performance perfectionism of the ATHLETE Questionnaire and disordered eating behaviors as measured by the EAT-26 score. Engaging in disordered eating behaviors and “personal expectation of superior athletic achievement and meeting the expectations of significant others” (15) are associated in the athletes.
The Pearson correlation coefficient for the “Support from teammates” subscale of the ATHLETE Questionnaire and the EAT-26 was r = .21, p = .093. This implies no relationship between support from teammates or the amount of trust in a teammate about disordered eating behaviors.
There was no significant correlation between the “Feelings about being an athlete” subscale and EAT-26 score, r = .12, p = .345. This demonstrates no significant relationship between the responses on the “Feelings about being an athlete” subscale of the ATHLETE Questionnaire and the EAT-26. This implies that among male high school runners, athletic identity has no relationship with runners engaging in disordered eating behaviors.
The Pearson correlation coefficient returned was r = .17, p = .167 for the “Physical Appearance” subscale of the EMI-2 and the EAT-26 score. This implies that motivation to exercise for physical appearance has no relationship with the likelihood of a male high school runner engaging in disordered eating behaviors.
The Pearson correlation coefficient for the “Feelings about Eating” subscale of The ATHLETE questionnaire and the EAT-26 score was r = .18, p = .137. This indicates no significant relationship between that the social pressure toward eating versus disordered eating behaviors in the athletes.
There was no significant correlation between the “Feelings about your body” subscale of the ATHLETE questionnaire and the score on the EAT-26, r = .19, p = .109. This suggests that body shape has no association with the disordered eating behaviors of male high school cross country runners.
DISCUSSION
Millions of people from all ages and genders in the U.S. suffer from eating disorders. Research has shown that females are at greater risk for eating disorders than males (17, 32, 39). Some studies have shown that athletes and adolescents in particular, are more susceptible to eating disorders than in non-athletic populations (28, 35). However, limited research about eating disorders is available in high school male cross country and distance runners.
Given the rising rates associated with eating disorders across all ages and genders and in particular adolescent males, understanding the prevalence with contributing factors was deemed necessary in a male athletic group. Therefore, the goals of this study were to determine the degree of disordered eating and contributing factors among high school male cross country runners.
The present study determined that 4.4% (n = 3) males scored 20 or higher on the EAT-26. A score of 20 or higher indicates an individual is at-risk for an eating disorder and displays symptoms. An additional 13.2% (n = 9) met the cut-off score of 14 for disordered eating behaviors. The results of the present study are in agreement with previous research that disordered eating among male athletes may be more of an issue than previously thought (10, 29, 30). Previous research on disordered eating behaviors in female athletes, using the EAT-26, revealed a mean score of 6.97 (SD = 6.99) (5). The present sample was similar for males (M = 6.04, SD = 6.52; N = 68). Although the EAT-26 cannot diagnose a particular eating disorder, the symptoms can be predictive of risk status. Much of the previous research deals with eating disorders in males of all ages, versus the adolescent male athletes in the present study. While previous research focused on other characteristics that may have had an impact on the higher prevalence rates, the current study focused on factors more specific to male adolescent athletes. These include the correlates of performance perfectionism, drive for thinness, and body dissatisfaction in athletes.
Modest positive correlation coefficients were found with the intra-individual characteristics on the EMI-2 and the ATHLETE questionnaires with overall EAT-26 scores. The “Your Body and Sports” subscale of the ATHLETE questionnaire measured drive for thinness and the connection to enhanced performance or appearance. This subscale included excessive or compulsive training above the requirement of the training program. The “Feelings about performance” subscale measured feelings toward performance perfectionism defined as “the excessive personal expectations for superior athletic performance and with respect to meeting expectations of significant others” (15). A higher mean score on “Your Body and Sports” and “Feelings about performance” subscales of the ATHLETE questionnaire and “Weight Management” subscale of the EMI-2 are indicative of greater degrees of the three constructs. The performance factor is associated with disordered eating behaviors by the “Your body and sports” and “Feelings about performance” subscales versus the overall EAT-26 score.
A higher mean score on the weight management subscale of the EMI-2 is related to weight management and motivation to exercise. The current study revealed 32% (n = 22) of male high school runners scored 3.25 or higher on the weight management subscale. This indicates perception of current weight as the items centered on “staying slim”, “losing weight”, or “burning calories” (20). A desire to control weight is associated with disordered eating behaviors in male high school cross country runners as determined from the modest correlation coefficient for the weight management subscale and the EAT-26 score.
Previous research (11) has suggested that males with disordered eating habits tended to exercise more for physical appearance reasons. The present study determined that 50% (n = 34) male high school runners scored 3.25 on the items in the physical appearance subscale of the EMI-2. This suggests that this group of athletes may exercise in order to “look more attractive”, “have a good body”, or “improve one’s body” (20). However, there was no significant correlation for the “Physical Appearance” subscale of the EMI-2 and the EAT-26 score. This suggests that although physical appearance may be desired, male high school runners exclude disordered eating behaviors for physical appearance as measured by the EAT-26.
Of the 68 participants in the study sample, 48 were White (70.6%), followed by Asian-American and Pacific Islander (11.8%, n = 8), 2 or more races (8.8%, n = 6), Hispanic and Latino (5.9%, n = 4), and African-American (2.9%, n = 2). This limitation may indicate that the results are generalizable only to school districts of similar size and demographic makeup. Further, the demographic makeup of the teams differs from the school district as a whole. For instance, the makeup of the school district is that of Hispanic and Latino (43.4%), White (30.2%), African-American (12.0%), Asian and Pacific Islander (8.1%), Multi-Racial (5.8 %), Native American, American Indian, and Alaskan Native (0.5%) (25). Therefore, demographic information on a larger scale of cross country teams may provide more information of the students participating in the sport.
Disordered eating behaviors may be more prevalent in both athletes and the general population versus previously thought. The research suggests that eating disorders among males are underreported (3, 10). Professionals estimate that in addition to diagnosed eating disorders, there are as many as 25 million more with disordered eating behaviors that remain sub-clinical or unreported (24). Therefore, underreporting by the athletes in the present study is plausible.
The questionnaires were completed on one occasion by runners during the summer prior to the start of the season. A longitudinal study over the course of the school year and across sports in which the runners participate (e.g., cross country and track and field) may yield different results. This might determine whether individual characteristics stabilize over time or are situational to the sport or feelings of the athlete at the time. Research suggests that longitudinal results may provide eating disorder prevalence rates for male participants similar to those for females (12, 13,16).
Sixty-eight high school male cross country runners participated in the present study. Among the male runners, twenty-six (38.2%) had a desire to increase body weight, although these athletes participated in a sport where a lean body type is more desirable. However, 26.5% (n = 18) of the high school male runners had a desire to decrease body weight. The results of the current study appear to concur with the results of previous studies involving high school male and female athletes and non-athletes (27, 33, 34). In particular, Hague (11) shows remarkably similar results in male Division III college athletes where 37% (n = 29) desired to lose weight and 38% (n =34) desired to gain weight, although a sport-by-sport breakdown was not conducted (11). The athletes in the previous investigations desired a change in body weight, where females typically desired weight loss while males generally desired weight gain. The reasons for a desired weight change may be gender-dependent and based on body satisfaction. Although the present study did not investigate the reasons for dissatisfaction with current weight status, future studies may seek more information relative to the reasons. For example, do male cross country runners feel a need to be more muscular? Do the bodies of male cross country runners not fit the ideal?
The present study was conducted on male cross country runners from 12 high schools in one large, urban school district. The study was limited by a low number of participants relative to the number of runners on the teams and number of high schools in the school district. Perhaps a larger and more diverse population of male runners would provide more information with respect to the research question. The complexity of disordered eating and contributing factors may limit the understanding. The results may contribute to the recognition by the athletes, coaches, athletic trainers, teachers, and parents that male athletes are vulnerable to eating disorders and disordered eating behaviors.
CONCLUSIONS
This study suggests that disordered eating behaviors in high school male cross country runners are related to contributing factors. Factors that have a significant relationship with disordered eating are performance and weight management. No significant relationships were found between disordered eating behaviors in male cross country athletes and personal body feelings, feelings about eating, and being an athlete. Signs and symptoms may be different between male and female athletes, while prevalence rates may be similar and related to the rate of reporting
APPLICATIONS IN SPORT
Most studies involving disordered eating behaviors have centered on females in general and female athletes in particular. Recognizing and identifying that disordered eating behaviors exist in males and may manifest differently can assist those directly involved with this group of athletes. Programs can be established to deal with the complexities of the issue especially among parents, coaches, trainers, counselors, and the athletes (26). Educating those directly involved with this group of athletes (coaches, parents, and trainers) may help deter these athletes from using disordered eating behaviors. Rather than equating thinness to performance, educating athletes about nutrition and healthful eating habits to demonstrate the positive impact these factors will make on performance is of critical importance.
ACKNOWLEDGMENTS
Many thanks to the caring professors at SUU who helped shape this paper. A special thanks to Dr. Julie Taylor and Dr. Brian Lyons for the advice and suggestions in the early stages of developing this research topic. Thank you to all the anonymous high school male cross country runners and the coaches who participated in this study.
REFERENCES
- American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: Author.
- American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed., text revision). Washington, DC: Author.
- Baum, A. (2006). Eating disorders in the male athlete. Sports Medicine, 36(1), 1-6.
- Braun, D. L., Sunday, S. R., Huang, A., & Halmi, K. A. (1999). More males seek treatment for eating disorders. International Journal of Eating Disorders, 25(4), 415-424.
- Coker, A. M. (2011). Coach pressure and disordered eating in female collegiate athletes: Is the coach-athlete relationship a mediating variable? (Master’s Thesis). Retrieved from ProQuest Dissertations and Theses database. (UMI No. 1497081)
- Doninger, G. L., Enders, C. K., & Burnett, K. F. (2005). Validity evidence for Eating Attitudes Test scores in a sample of female college athletes. Measurement in Physical Education and Exercise Science, 9(1), 35-49.
- Fulkerson, J. A., Keel, P. K., Leon, G. R., & Dorr, T. (1999). Eating-disordered behaviors and personality characteristics of high school athletes and nonathletes. International Journal of Eating Disorders,26(1), 73-79.
- Furnham, A., Badmin, N., & Sneade, I. (2002). Body image dissatisfaction: Gender differences in eating attitudes, self-esteem, and reasons for exercise. The Journal of Psychology, 136(6), 581-596.
- Garner, D. M., Olmstead, M. P., Bohr, Y., & Garfinkel, P. E. (1982). The Eating Attitudes Test: Psychometric features and clinical correlates. Psychological Medicine, 12,871-878.
- Glazer, J. L. (2008). Eating disorders among male athletes. Current Sports Medicine Reports, 7(6), 332- 337.
- Hague, C. (2010). Differences between male and female division III athletes in eating attitudes, body perception, and reason for exercise. Retrieved from http://hdl.handle.net/10090/16482
- Halvorsen, J. (2003). Longitudinal examination of disordered eating correlates in collegiate female gymnasts (Unpublished Master’s Thesis). Retrieved from http://etd.fcla.edu/UF/UFE0001160/halvorsen_j.pdf
- Hausenblas, H. A., & Carron, A. (1999). Eating disorder indices and athletes: An integration. Journal of Sport & Exercise Psychology, 21(3), 230-258.
- Hausenblas, H. A., & McNally, K. D. (2004). Eating disorder prevalence and symptoms for track and field athletes and nonathletes. Journal of Applied Sport Psychology, 16, 274-286.
- Hinton, P., & Kubas, K. (2005). Psychosocial correlates of disordered eating in female collegiate athletes: Validation of the ATHLETE questionnaire. Journal of American College Health, 54(3), 149-156. doi:10.3200/JACH.54.3.149-156.
- Keel, P. K., Klump, K. L., Leon, G. R., Fulkerson, J. A. (1998). Disordered eating in adolescent males from a school-based sample. International Journal of Eating Disorder, 23(2), 125-132.
- Kjelsas, E., Bjornstrom, C., & Gotestam, K. G. (2004). Prevalence of eating disorders in female and male adolescents (14-15 years). Eating Behaviors, 5(1), 13-25.
- Koszewski, W., Chopak, J., & Buxton, B. (1997). Risk factors for disordered eating in athletes. Athletic Therapy Today, 2(2), 7-11. Retrieved from Academic Search Premier database.
- Lewisohn, P. M., Seeley, J. R., Moerk, K. C., Stiegel-Moore, R. H. (2002). Gender differences in eating disorder symptoms in young adults. International Journal of Eating Disorders, 32(4), 426-440.doi:10.1002/eat.10103
- Markland, D., & Ingledew, D. K. (1997). The measurement of exercise motives: Factorial validity and invariance across gender of a revised Exercise Motivations Inventory. British Journal of Health Psychology, 2, 361-376.
- McClure, A. J. (1997). The prevalence of eating disorders within Division I and Division III intercollegiate athletics(Master’s Thesis). Retrieved from Kinesiology Publications. (SPH450039).
- Milligan, B., & Pritchard, M. E. (2006). The relationship between gender, sport, self-esteem and eating disordered behaviors in Division I athletes. Athletic Insight, 8(1), 9-43.
- Mintz, L. B., & O’Halloran, M. S (2000). The eating attitudes test: Validation with the DSM-IV eating disorder criteria. Journal of Personality Assessment, 74(3), 489-503.
- National Association of Anorexia Nervosa and Associated Disorders. (2010). Facts about Eating Disorders. Retrieved from http://www.anad.org/get-information/about-eating-disorders/eating-disorders-statistics/
- Nevada Department of Education Office of Public Instruction. (2012). Nevada Annual Reports of Accountability. [Data File]. Retrieved from http://www.nevadreportcard.com/profile/overview.aspx?levelid=D&entityid=02&yearid=11-12
- O’Dea, J. A., & Abraham, S. (2000). Improving the body image, eating attitudes, and behaviors of young male and female adolescents: A new educational approach that focuses on self-esteem. International Journal of Eating Disorders, 28(1), 43-57.
- Parks, P. S., & Read, M. H. (1997). Adolescent male athletes: Body image, diet, and exercise. Adolescence (Fall), 32(127), 593-602.
- Patel, D. R., Pratt, H. D., & Greydanus, D. E. (2003). Treatment of adolescents with anorexia nervosa. Journal of Adolescent Research, 18(3), 244-260. doi: 10.1177/0743558403018003004
- Petrie, T. A., & Rogers, R. (2001). Extending the discussion of eating disorders to include men and athletes. The Counseling Psychologist, 29(5), 743-753. doi: 10.1177/0011000001295006
- Petrie, T. A., Greenleaf, C. A., Carter, J. E., & Reel, J. (2007). Psychosocial correlates of disordered eating among male collegiate athletes. [Abstract]. Journal of Clinical Sport Psychology, 1(4), 340-357.
- Pritchard, M., Rush, P., & Milligan, B. (2007). Risk factors for disordered eating in high school and college athletes. Athletic Insight, 9(3). Retrieved from http://www.athleticinsight.com/Vol9Iss3/EatingDisorderRiskFactors.htm
- Smolak, L., Murnen, S. K., & Ruble, A. E. (2000). Female athletes and eating problems: A meta-analysis. International Journal of Eating Disorders, 27(4), 371-380.
- 33. Sundgot-Borgen, J., & Torstveit, M. K. (2004). Prevalence of eating disorders in elite athletes is higher than in the general population. Clinical Journal of Sport Medicine, 14(1), 25-32.
- Taub, D. E., & Benson, R. A. (1992). Weight concerns, weight control techniques, and eating disorders among adolescent competitive swimmers: The effect of gender. Sociology of Sport Journal, 9(1), 76-86.
- Thompson, R. A., & Sherman, R. T. (1999). Athletes, athletic performance, and eating disorders: Healthier alternatives. Journal of Social Issues, 55(2), 317-337.
- Thompson, R. A., & Sherman, R. T. (2005). The last word. Eating Disorders, 13(3), 321-324. doi: 10.1080/10640260590932922
- 37. Wimbish, T. (2009). Eating disorders, body-image dissatisfaction, and drive for muscularity in African American gay and straight men (Doctoral dissertation). Retrieved from ProQuest. (AAT3391518).
- 38. Wiseman, C. V., Peltzman, B., Halmi, K. A., & Sunday, S. R. (2004). Risk factors for eating disorders: Surprising similarities between middle school boys and girls. Eating Disorders, 12, 315-320. doi: 10.1080/10640260490521398
- 39. Woodside, D. B, Garfinkel, P. E., Lin, E.,Goering, P., Kaplan, A. S., Goldbloom, D. S., & Kennedy, S. H. (2001). Comparisons of men with full or partial eating disorders, men without eating disorders, and women with eating disorders in the community. The American Journal of Psychiatry, 158(4), 570-574.
FIGURES AND TABLES
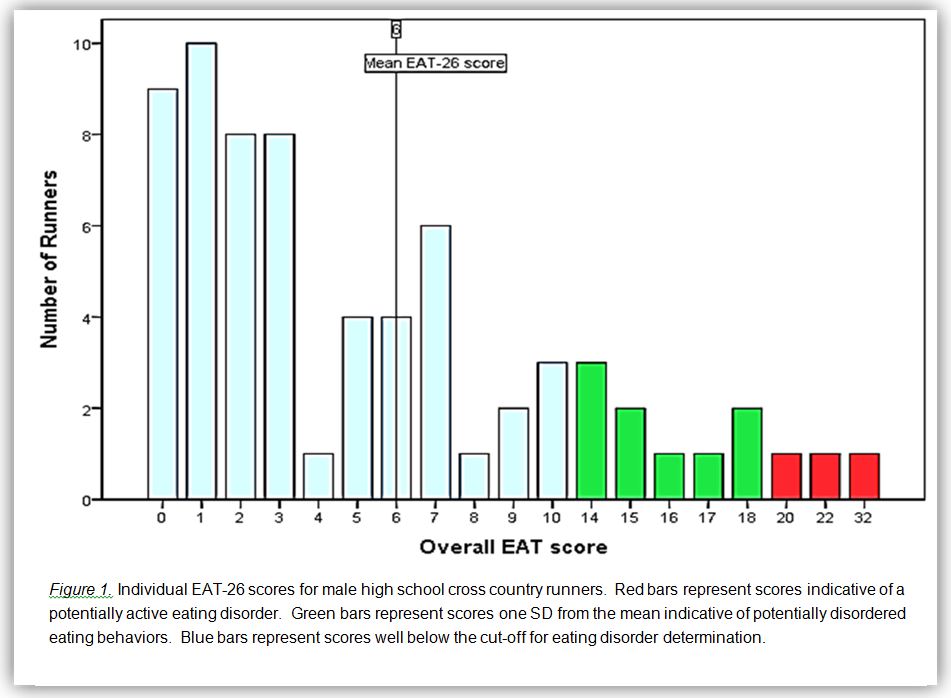
Table 1.
Demographic information
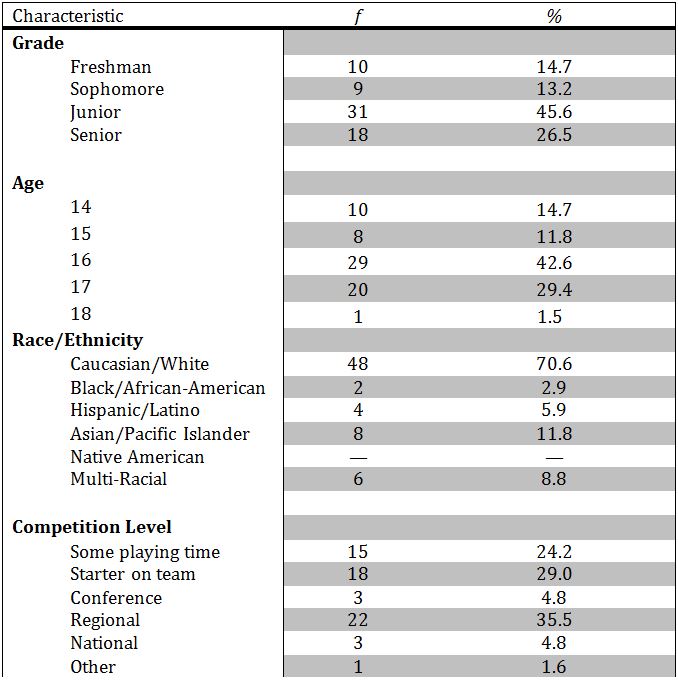
Note: Six athletes did not complete the competition level item on the questionnaire.
Table 2.
Descriptive statistics for the ATHLETE and EMI-2 questionnaires
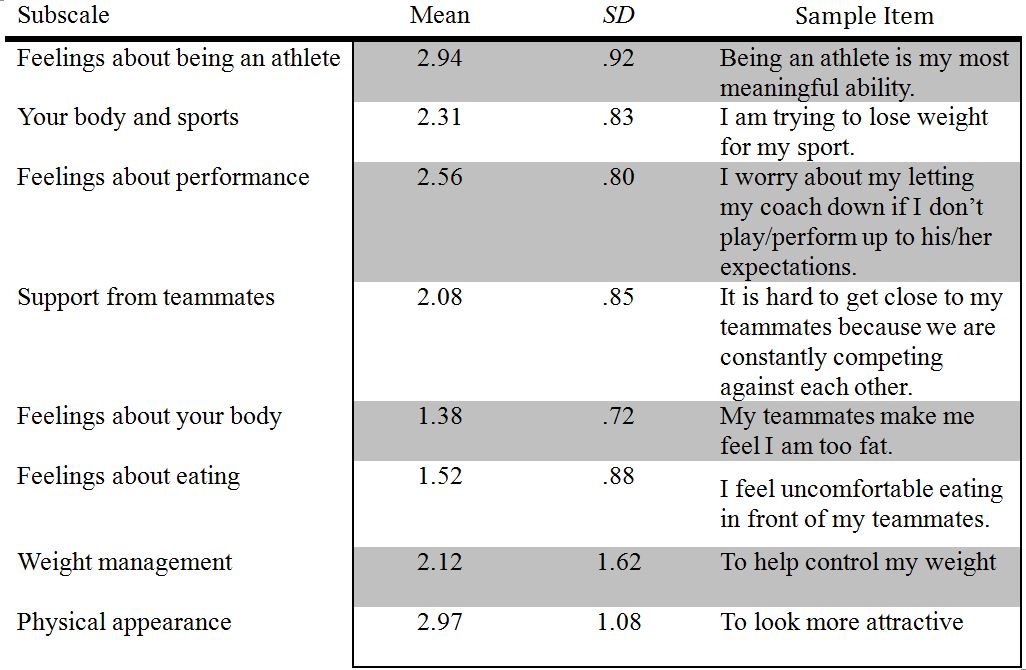
Note: Mean scores were determined by summing the scores for each subscale and dividing by the number of items in each subscale for each athlete. The maximum score for each item is five.
Table 3.
Responses to desired weight question on the ATHLETE questionnaire
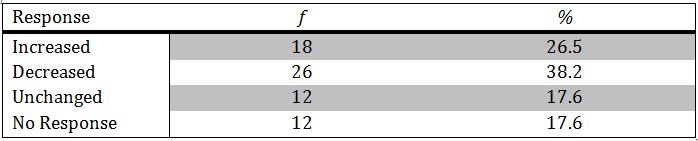
Note: Athletes were asked about current and desired weight and family weight history.
Table 4.
Correlations between EAT-26 scores and the ATHLETE and EMI-2 subscale scores
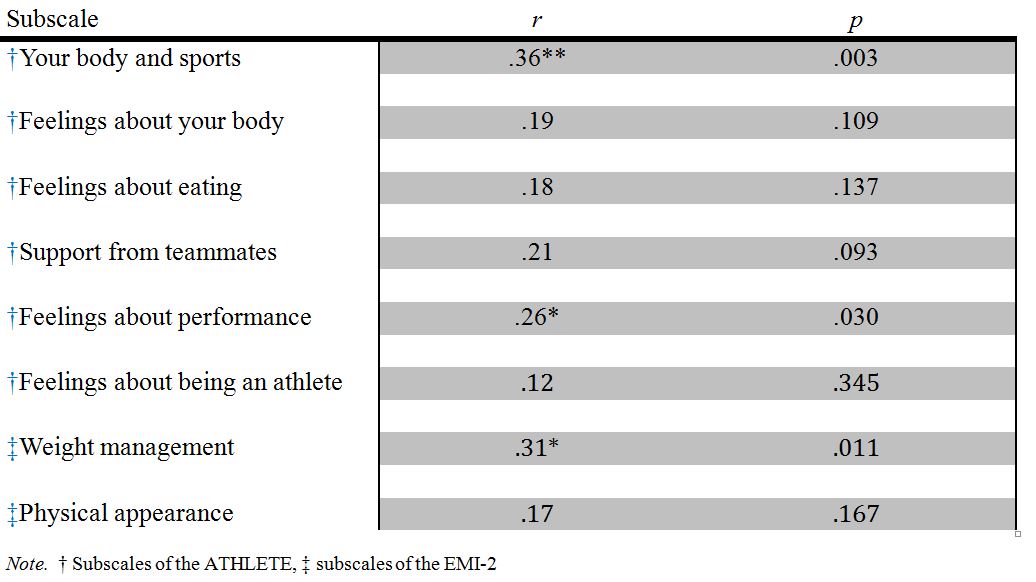
Note. † Subscales of the ATHLETE, ‡ subscales of the EMI-2
